Signal-Average Electrocardiogram
(Signal-Averaged ECG, Signal-Averaged EKG, SAECG)
What is a signal-averaged electrocardiogram?
An electrocardiogram (ECG or EKG) is one of the simplest and fastest procedures used to evaluate the heart. Electrodes (small, plastic patches) are placed at certain locations on the chest, arms, and legs. When the electrodes are connected to an ECG machine by lead wires, the electrical activity of the heart is measured, interpreted, and printed out for the physician's information and further interpretation.
A signal-averaged electrocardiogram is a more detailed type of ECG. During this procedure, multiple ECG tracings are obtained over a period of approximately 20 minutes in order to capture abnormal heartbeats which may occur only intermittently. A computer captures all the electrical signals from the heart and averages them to provide the physician more detail regarding how the heart’s electrical conduction system is working.
Signal-averaged ECG is one of several procedures used to assess the potential for dysrhythmias/arrhythmias (irregular heart rhythms) in certain medical situations.
Other related procedures that may be used to assess the heart include resting electrocardiogram (ECG), Holter monitor, exercise electrocardiogram (ECG), cardiac catheterization, chest x-ray, computed tomography (CT scan) of the chest, echocardiography, electrophysiological studies, magnetic resonance imaging (MRI) of the heart, myocardial perfusion scans, radionuclide angiography, and ultrafast CT scan. Please see these procedures for additional information.
The heart's electrical conduction system:
The heart is, in the simplest terms, a pump made up of muscle tissue. Like all pumps, the heart requires a source of energy in order to function. The heart's pumping action comes from an intrinsic electrical conduction system.
An electrical stimulus is generated by the sinus node (also called the sinoatrial node, or SA node), which is a small mass of specialized tissue located in the right atrium (right upper chamber) of the heart.
The sinus node generates an electrical stimulus regularly at 60 to 100 times per minute under normal conditions. This electrical stimulus travels down through the conduction pathways (similar to the way electricity flows through power lines from the power plant to your house) and causes the heart's lower chambers to contract and pump out blood. The right and left atria (the two upper chambers of the heart) are stimulated first and contract a short period of time before the right and left ventricles (the two lower chambers of the heart).
The electrical impulse travels from the sinus node to the atrioventricular (AV) node, where impulses are slowed down for a very short period, then continues down the conduction pathway via the “bundle of His” into the ventricles. The “bundle of His” divides into right and left pathways to provide electrical stimulation to both ventricles.
This electrical activity of the heart is measured by an electrocardiogram. By placing electrodes at specific locations on the body (chest, arms, and legs), a graphic representation, or tracing, of the electrical activity can be obtained. Changes in an EKG from the normal tracing can indicate one or more of several heart-related conditions.
Reasons your physician may request a signal-averaged ECG may include, but are not limited to, the following:
-
to determine the cause of chest pain
-
to evaluate other signs and symptoms which may be heart-related, such as fatigue, shortness of breath, dizziness, or fainting
-
to help identify irregular heartbeats
-
for further evaluation of dysrhythmias/arrhythmias noted on resting ECG
There may be other reasons for your physician to recommend a signal-averaged ECG.
A signal-averaged ECG is a quick, noninvasive method of assessing the heart’s function. Risks associated with ECG are minimal and rare.
Prolonged application of the adhesive electrode patches may cause tissue breakdown or skin irritation at the application site.
There may be other risks depending upon your specific medical condition. Be sure to discuss any concerns with your physician prior to the procedure.
Certain factors or conditions may interfere with or affect the results of the test. These include, but are not limited to, the following:
-
obesity, pregnancy, or ascites (accumulation of fluid in the abdomen)
-
anatomical considerations such as the size of the chest and the location of the heart within the chest
-
movement during the procedure
-
exercise, intake of high-carbohydrate meal, and/or smoking prior to the procedure
-
certain medications
-
electrolyte abnormalities, such as too much or too little potassium, magnesium, and/or calcium in the blood
-
Your physician or the technician will explain the procedure to you and offer you the opportunity to ask any questions that you might have about the procedure.
-
Generally, fasting is not required before the test.
-
Notify your physician of all medications (prescribed and over-the-counter) and herbal supplements that you are taking.
-
Notify your physician if you have a pacemaker.
-
The area(s) where the electrodes are to be placed may be shaved.
-
Based upon your medical condition, your physician may request other specific preparation.
A signal-averaged ECG may be performed on an outpatient basis or as part of your stay in a hospital. Procedures may vary depending on your condition and your physician’s practices.
Generally, a signal-averaged ECG follows this process:
-
You will be asked to remove any jewelry or other objects that may interfere with the procedure.
-
You will be asked to remove clothing from the waist up. The technician will ensure your privacy by covering you with a sheet or gown and exposing only the necessary skin.
-
You will lie flat on a table or bed for the procedure. It will be important for you to lie still and not talk during the procedure, so as not to interfere with the tracing.
-
If your chest is very hairy, the technician may shave small patches of hair, as needed, so that the electrodes will stick closely to the skin.
-
Electrodes will be attached to your chest, abdomen, and back.
-
The lead wires will be attached to the skin electrodes.
-
Once the leads are attached, the technician may key in identifying information about you into the machine's computer.
-
The EKG will be started. Generally, it will take about 20 minutes to obtain the necessary ECG information.
-
Once the tracing is completed, the technician will disconnect the leads and remove the skin electrodes.
You should be able to resume your normal diet and activities, unless your physician instructs you differently.
Generally, there is no special care following a signal-averaged ECG.
Notify your physician if you develop any signs or symptoms you had prior to the test (e.g., chest pain, shortness of breath, dizziness, or fainting).
Your physician may give you additional or alternate instructions after the procedure, depending on your particular situation.







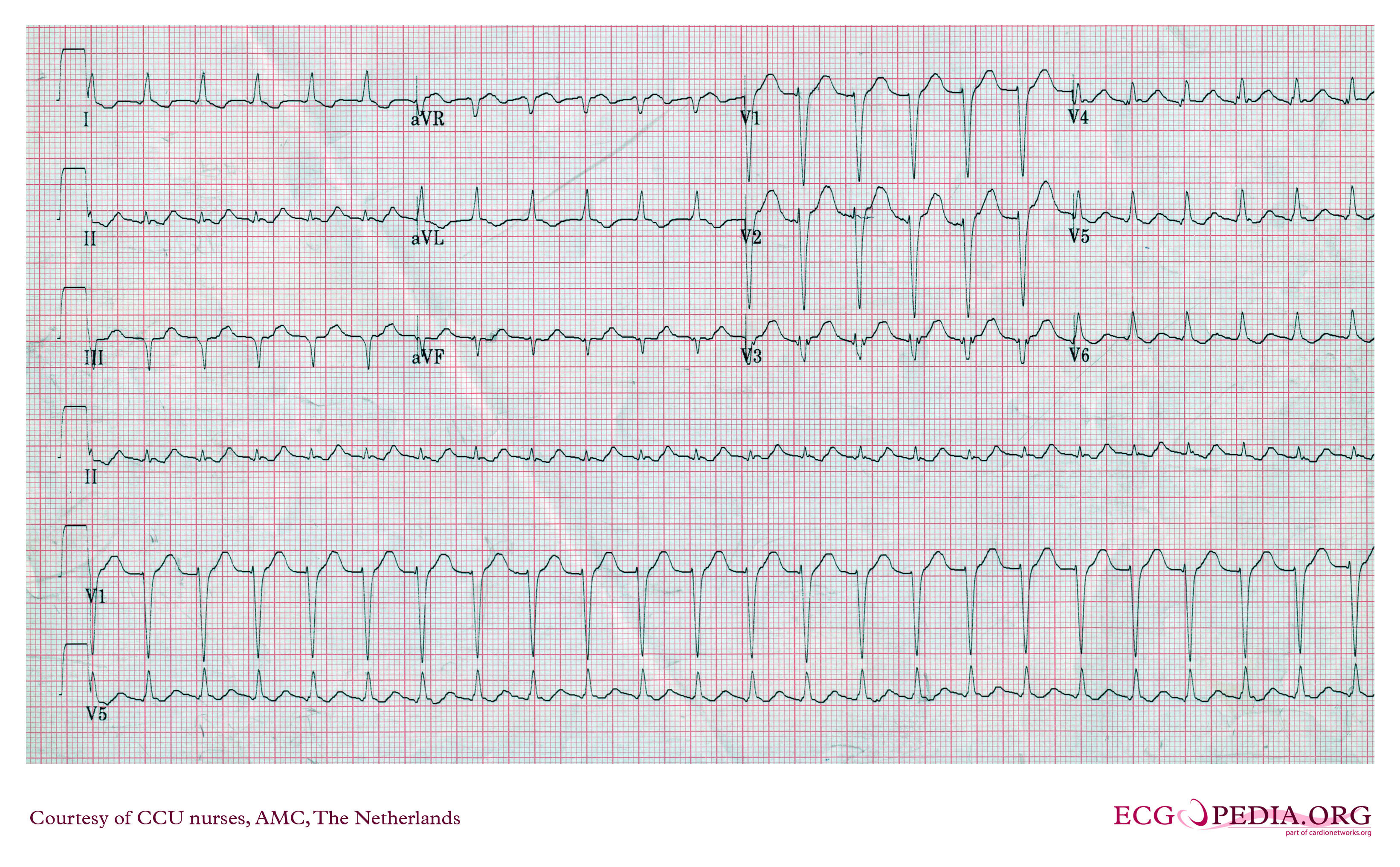
 shows an ECG from a 29-year patient with PJRT. The tachycardia was an incidental finding on a routine ECG and the patient was asymptomatic. The tachycardia is described as a long RP tachycardia (see below). The p wave looks different to sinus rhythm – it is typically inverted in the inferior leads (II, III and aVF) - indicating atrial activation from “low to high” (the opposite direction to sinus rhythm). The p-R interval is typically relatively normal
shows an ECG from a 29-year patient with PJRT. The tachycardia was an incidental finding on a routine ECG and the patient was asymptomatic. The tachycardia is described as a long RP tachycardia (see below). The p wave looks different to sinus rhythm – it is typically inverted in the inferior leads (II, III and aVF) - indicating atrial activation from “low to high” (the opposite direction to sinus rhythm). The p-R interval is typically relatively normal 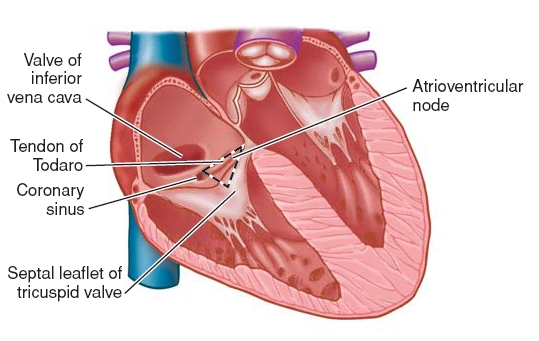






 خوشبختى لذت مشتركى است كه حاصل يارى بى چشمداشت به ديگران است .
خوشبختى لذت مشتركى است كه حاصل يارى بى چشمداشت به ديگران است .{kind=link}